*Online Consultations Available

*Online Consultations Available
1,000+ Shoulder Surgeries performed
Rehab-IntegratedâĻ
Care
Outcomes Tracked for 5 Years
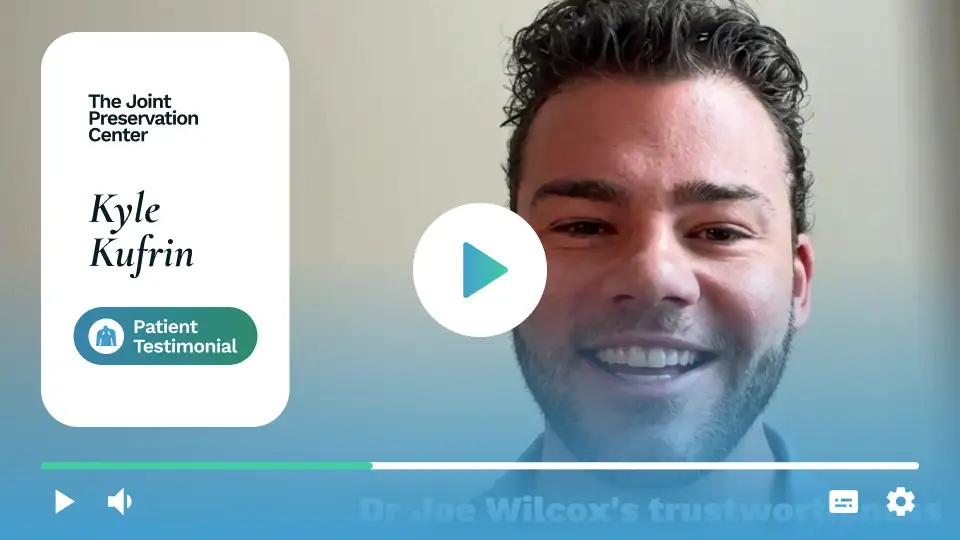


Subacromial impingement occurs when the space between the top of your shoulder (the acromion) and the rotator cuff tendons beneath it becomes too narrow â compressing the tendons and bursa with every arm movement.
Â
X-ray and MRI reports can describe impingement-related findings across five key factors. Understanding what your imaging shows helps clarify why conservative care may not be resolving your pain â and what surgical correction can address.
The acromion is the bony roof of the shoulder. Its shape is one of the strongest predictors of structural outlet impingement and surgical candidacy.

A. Type I (Flat) Acromion
A flat undersurface that allows adequate clearance for the rotator cuff tendons. Structural impingement is less likely from acromion shape alone.



Bone spurs (osteophytes) on the undersurface of the acromion or the acromioclavicular (AC) joint are a common cause of mechanical outlet narrowing.
On X-ray, the subacromial space â the gap between the humeral head and the acromion â can be measured. Narrowing below approximately 7 mm is associated with impingement and rotator cuff pathology.
Â

The subacromial-subdeltoid bursa is a fluid-filled sac that cushions the rotator cuff tendons beneath the acromion. MRI reliably characterizes bursal involvement.
Â

Chronic subacromial impingement places repeated stress on the supraspinatus tendon, which runs directly beneath the acromion. MRI reveals the degree of tendon involvement.
Â

Calcium hydroxyapatite deposits can form within the rotator cuff tendons â most commonly the supraspinatus â producing a distinct condition called calcific tendinitis. Although often associated with impingement, calcific tendinitis can occur in isolation.
Surgical calcium removal is typically appropriate when barbotage, cortisone, shockwave therapy (ESWT), and PRP have failed to provide meaningful or lasting relief. Arthroscopic calcium removal is highly effective, with excision of the deposit and lavage of the area under direct visualization.

*Same-day consultations may be available


Even when X-ray confirms a hooked acromion or bone spur, and MRI confirms bursitis or tendon involvement, imaging does not define the complete clinical picture. Subacromial impingement must be interpreted in the context of your strength, range of motion, occupational demands, prior treatment history, and how symptoms have changed over time.
Â
A shoulder specialist integrates these factors through comprehensive evaluation before defining the most appropriate path forward â including whether arthroscopic decompression is indicated and which structures require addressing.

Rarely, without addressing the underlying structural cause.
Â
Structural impingement caused by a hooked acromion, bone spur, or os acromiale does not correct itself over time. The mechanical narrowing remains, and continued overhead loading perpetuates tendon and bursa compression. While symptoms may temporarily fluctuate, the underlying anatomy does not change without intervention. For patients with calcific tendinitis, small deposits occasionally reabsorb spontaneously, but medium and large deposits are unlikely to resolve without procedural intervention. A comprehensive evaluation will determine whether your specific impingement pattern has a realistic chance of conservative resolution or whether the structural cause requires correction.
Subacromial impingement varies in its behavior. Some patients remain stable with conservative management for extended periods; others experience gradual worsening despite ongoing treatment.
Â
Risk of progression increases with structural severity (hooked acromion, large bone spurs), ongoing overhead occupational or athletic demands, and the duration of failed conservative care. The most significant clinical concern is that chronic mechanical impingement can cause direct damage to the underlying rotator cuff tendons â turning a structural problem into a combined structural and tendon pathology that requires more complex surgical management.

As impingement continues without treatment:
Functional progression in daily life:
Occupational and sport impact:
For working-age adults in overhead occupations or overhead sports, delay in addressing the structural cause of impingement can translate directly into extended time away from work and reduced earning capacity â in addition to the risk of developing a more complex surgical condition.

Subacromial impingement is unique among shoulder conditions: surgical candidacy is almost entirely defined by conservative treatment failure. Most patients who reach the decision to consider surgery have already committed to physical therapy for months, received multiple cortisone injections, and tried activity modification â without achieving lasting relief.
Â
This is not a failure on your part. It reflects the nature of structural impingement: when the mechanical cause is an acromial bone spur, a hooked acromion, or a thickened coracoacromial ligament, no amount of rehabilitation can reshape bone or remove the impinging structure. Non-surgical care can reduce inflammation and improve shoulder mechanics around the obstruction â but it cannot eliminate the obstruction itself.
Physical therapy has not produced lasting improvement. If six or more weeks of structured, progressive rehabilitation has failed to meaningfully reduce pain or restore function, the structural cause of impingement is likely preventing further gains.
Â
Cortisone injections are wearing off faster. An injection that once provided months of relief now lasts weeks â or no longer provides meaningful improvement at all. Increasing injection frequency or diminishing duration are recognized clinical signals of conservative care failure.
Â
You have had three or more cortisone injections. Repeated injections carry cumulative risks to tendon tissue. Most guidelines recommend considering surgical evaluation after three injections without sustained benefit.
Â
Barbotage or shockwave therapy has not resolved calcific deposits. For calcific tendinitis specifically, failure of needling and lavage (barbotage), extracorporeal shockwave therapy (ESWT), or PRP injection indicates that arthroscopic calcium removal is the appropriate next step.
Â
Pain is affecting your ability to work or perform overhead tasks. Occupational impairment â inability to perform your job reliably due to shoulder pain â is one of the strongest indicators that surgical decompression is warranted.
Â
You have tried everything and remain in pain. Failure of multiple conservative modalities â PT, injections, anti-inflammatories, activity modification, rest â in combination defines the patient population most likely to benefit from surgical decompression.
Physical therapy CAN:
Physical therapy CANNOT:
For working adults and overhead athletes, the practical question is straightforward: is your shoulder meeting the demands of your work, your sport, and your life? If it is not â and if conservative care has not been able to restore that function â a surgical evaluation is a reasonable and often overdue step.

Appropriate treatment for subacromial impingement depends on the structural cause, the degree of conservative care failure, the condition of the rotator cuff tendons, and the occupational and athletic demands placed on your shoulder.
For patients in the early stages of impingement â without confirmed structural outlet obstruction or significant conservative care failure â structured physical therapy may reduce pain and improve function. It is the appropriate starting point before surgical evaluation for most patients.


Physical therapy alone may be less appropriate when:
Â
Â
For overhead workers, tradespeople, and athletes, the threshold for surgical evaluation is often practical: when the shoulder can no longer reliably perform the demands of the job or sport, and conservative care is not restoring that capacity, arthroscopic decompression offers a direct structural solution.

Who Is a Candidate?
Â
Arthroscopic subacromial decompression is the primary surgical treatment for structural outlet impingement. Candidates typically have:
Â
Â
What the Procedure Involves
Â
Arthroscopic subacromial decompression is performed through small keyhole incisions using a specialized camera and instruments. The procedure is typically performed under regional anesthesia with sedation or general anesthesia and takes approximately 30â60 minutes for a straightforward decompression.
Â
During the procedure:
Â
Â
Recovery
Â
Subacromial decompression has a substantially faster recovery than rotator cuff repair because no tendon is being reattached to bone.
Â
Â
Most patients experience progressive pain improvement beginning within the first 2â4 weeks, with functional overhead capacity continuing to improve over 3â6 months as rehabilitation restores strength and endurance.

Who Is a Candidate?
Â
Bursectomy â surgical removal of the inflamed subacromial bursa â is performed as part of arthroscopic decompression in most cases. When significant bursitis exists without a prominent structural bone spur, bursectomy alone (without acromioplasty) may be considered. Candidates include patients with:
Â
Â
What the Procedure Involves
Â
The inflamed bursa is visualized arthroscopically and removed using a motorized shaver. This eliminates the chronic inflammatory tissue that has been generating pain and is no longer responsive to conservative management. When performed alongside acromioplasty, bursectomy is part of the same arthroscopic procedure with no additional incisions.
Â
Recovery
Â

The coracoacromial ligament forms the anterior border of the subacromial outlet. When thickened or pathologically tight, it contributes to dynamic impingement â particularly with forward flexion and internal rotation. CAL release is routinely performed as part of arthroscopic decompression and does not significantly add to recovery time. It is rarely performed as a standalone procedure.

Who Is a Candidate?
Â
Arthroscopic calcium removal is indicated for patients with calcific tendinitis whose calcium deposits have not resolved with conservative care. Surgical candidates typically have:
Â
Â
What the Procedure Involves
Â
Arthroscopic calcium removal is performed through the same small incisions used for standard shoulder arthroscopy. Under direct visualization, the calcium deposit is located, the tendon is carefully incised, and the calcium material is evacuated and lavaged. When associated impingement or bursitis is present, decompression and bursectomy are performed in the same procedure.
Â
Success rates for arthroscopic calcium removal are high, with the majority of patients experiencing significant and durable pain relief following surgery after failed conservative care.
Â
Recovery
Â


Subacromial impingement rarely occurs in complete isolation. MRI frequently reveals concurrent pathology that contributes to shoulder pain and dysfunction. When multiple structures are compromised, addressing only the impingement may leave residual symptoms. At The Joint Preservation Center, we evaluate the full spectrum of shoulder pathology and address all relevant structures in a single arthroscopic procedure where possible.
Decompression with rotator cuff repair is the most common combined procedure in shoulder surgery. Chronic subacromial impingement is a leading cause of rotator cuff tears, as mechanical abrasion from a bone spur or hooked acromion gradually damages the supraspinatus tendon over time. When MRI shows both structural impingement and a significant partial or full-thickness rotator cuff tear, decompression alone is insufficient. Arthroscopic subacromial decompression removes the structural cause while concurrent rotator cuff repair restores tendon integrity, both performed through the same small incisions in a single operation. Recovery follows the rotator cuff repair timeline, as tendon-to-bone healing governs the rehabilitation schedule.

AC joint bone spurs or AC joint arthritis can project downward into the subacromial space, contributing to impingement independently of acromion morphology. When imaging or intraoperative findings confirm symptomatic AC joint pathology alongside impingement, distal clavicle excision (removal of a small portion of the end of the clavicle) can be performed arthroscopically during the same operation. This addresses the AC joint contribution to subacromial narrowing and eliminates AC joint-generated pain simultaneously.

The long head of the biceps tendon passes through the shoulder joint and can become a source of concurrent pain in impingement patients â particularly when biceps tendinopathy, partial tearing, or instability is present alongside bursitis and outlet narrowing.
Â
When biceps pathology is identified, biceps tenodesis â detaching the damaged tendon from its anchor inside the joint and securing it to a new position on the humerus â eliminates the intra-articular pain source while preserving biceps strength and cosmesis. This is performed arthroscopically at the time of subacromial decompression, avoiding a second surgical procedure.

In some patients, structural impingement, calcific deposits, and chronic bursitis coexist. Each component is addressed during the same arthroscopic procedure: acromioplasty removes the structural outlet obstruction, arthroscopic calcium removal eliminates the calcific deposit, and bursectomy removes the chronically inflamed bursal tissue. Combining these procedures avoids multiple surgeries and typically does not significantly extend recovery beyond what any single procedure would require.

A subacromial decompression that provides initial improvement but then fails â through recurrence of bone formation (bone regrowth), inadequate initial resection, or progression of concurrent rotator cuff pathology â may require revision surgery.
Â
When revision is indicated, we evaluate the original imaging, operative records, and current MRI to identify the source of symptom recurrence. Revision decompression may involve completing an inadequate initial resection, addressing bone regrowth at the acromioplasty site, or managing concurrent pathology (rotator cuff tear, biceps involvement) that was not addressed at the primary procedure.
Recovery after arthroscopic subacromial decompression is significantly faster than recovery after rotator cuff repair, because no tendon is being reattached to bone. The primary goals of early recovery are pain control, reducing post-surgical inflammation, and beginning rehabilitation to restore range of motion and strength.
Â
Recovery timelines vary depending on whether decompression was performed alone or in combination with rotator cuff repair, biceps tenodesis, or AC joint procedures. Your surgeon will guide you through a protocol tailored to the specific procedures performed.
Phase 1: Early Recovery (Weeks 0â2)
Sling use for comfort only. Pain management with medication and icing. Gentle pendulum exercises and early passive motion begin within the first 48â72 hours. Most patients notice significant improvement in acute post-operative discomfort within the first 5â7 days.
Â
Phase 2: Active Motion (Weeks 2â6)
Active range-of-motion exercises begin as pain allows. Overhead reaching tolerance increases progressively. Most patients regain near-full range of motion by weeks 4â6 after isolated decompression.
Â
Phase 3: Strengthening (After ~6 Weeks)
Controlled strengthening of the rotator cuff, deltoid, and scapular stabilizers begins. This phase progressively rebuilds the strength and endurance needed for overhead work and overhead sport.
Â
If rotator cuff repair is performed simultaneously, rehabilitation progresses according to the rotator cuff repair protocol, which is longer and more protective of the healing tendon.

Drive?
Usually when you are out of the sling and off narcotic pain medication â typically within 1â2 weeks for isolated decompression.
Â
Return to desk work?
Often within 1â2 weeks, depending on comfort and pain medication use.
Â
Return to light overhead activity?
Typically 4â6 weeks.
Â
Return to manual labor, construction, or trades?
Typically 3â4 months after decompression alone; longer if rotator cuff repair is combined.
Â
Return to overhead sports?
Approximately 3â5 months for most overhead activities. Pitching, swimming, and CrossFit overhead movements may require 4â6 months.
One of the most common concerns for working adults and tradespeople considering shoulder decompression surgery is timing: how to schedule the procedure to minimize income disruption and plan for the recovery period.
Â
Desk work and computer-based roles: Most patients return within 1â2 weeks, working with the operated arm supported or minimally loaded. Remote work may allow even earlier transition.
Â
Supervisory, client-facing, or managerial roles: Return within 1â2 weeks is typical if physical lifting is not required.
Â
Construction, painting, electrical, plumbing, roofing, and overhead trades: Return to light duty may be possible within 4â6 weeks. Return to full overhead work typically requires 3â4 months. Modified duty during recovery â ground-level tasks, supervisory roles â can minimize income impact significantly.
Â
Athletes and coaches: Return to sport-specific training typically begins at 3â4 months, with full competitive return at 4â6 months depending on sport.
Â
Workers’ Compensation: For patients with occupational shoulder injuries, we provide work restriction documentation and return-to-work clearance letters as needed for employers, occupational health departments, and workers’ compensation case managers.
Â
Patients who plan ahead consistently report a smoother, less stressful early recovery.
Recovery timelines vary based on whether additional procedures were performed. This timeline applies to arthroscopic decompression without concurrent rotator cuff repair.
Â
Week 1: Sling for comfort. Pain management with medication and icing. Pendulum exercises begin. Most acute post-operative pain resolves significantly by day 5â7.
Â
Weeks 2â3: First post-operative visit. Active-assisted range-of-motion exercises begin. Desk work resumes if comfortable. Sling discontinued when no longer needed for comfort.
Â
Weeks 4â6: Progressive active range of motion. Overhead tolerance increasing. Driving typically possible by week 2â3 after sling is discontinued.
Â
Weeks 6â10: Strengthening phase begins. Rotator cuff and scapular stabilizer exercises. Daily activities become noticeably easier. Light occupational tasks may resume depending on demands.
Â
Months 3â4: Return to overhead work and overhead sport for most patients. Progressive return to full occupational demands.
Â
Months 4â6: Full strength and endurance recovery. Return to competitive overhead sport and full-duty overhead occupational work.
Â
If rotator cuff repair is performed simultaneously, recovery follows the rotator cuff repair timeline (see rotator cuff tear page).

Modern arthroscopic stabilization techniques are associated with:
High rates of re-dislocation prevention
Significant gains in shoulder confidence and function
Improved functional outcome scores
High patient satisfaction
1
We evaluate your symptoms, shoulder strength and movement, review your X-ray and MRI, and discuss your occupational demands, activity level, and prior treatment history. If imaging has not been obtained, we can order X-ray and MRI.
2
We explain whether continued rehabilitation, additional non-surgical care, or arthroscopic surgical decompression is appropriate based on your imaging findings, clinical examination, and treatment history.
3
If surgery is recommended, our fellowship-trained shoulder surgeons performs arthroscopic subacromial decompression â acromioplasty, bursectomy, and any additional procedures indicated by your imaging â through small keyhole incisions to create lasting relief.
4
Our surgeons work closely with physical therapists to guide a progressive rehabilitation program that restores overhead strength and function while allowing the shoulder to heal properly.
5
Rehabilitation progresses through milestones so you can confidently return to the overhead activities that matter most â your trade, your sport, or the daily tasks that impingement has been limiting.
This long-term follow-up helps us understand how shoulders recover beyond the early healing period â including pain resolution, strength restoration, return to overhead work, and return to sport. These insights allow our surgeons to continually refine surgical planning and rehabilitation strategies to support durable shoulder performance over time.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
Subacromial impingement syndrome occurs when the rotator cuff tendons and subacromial bursa are compressed between the humeral head and the bony roof of the shoulder (acromion). With every forward arm movement or overhead lift, the tendons and bursa must pass through the subacromial space, and when that space is mechanically narrowed by a hooked acromion, bone spur, thickened coracoacromial ligament, or swollen bursa, repeated friction and compression produce pain, inflammation, and over time potential tendon damage. Impingement is not a single diagnosis but a spectrum, and the appropriate treatment depends on the specific cause and severity of the narrowing, the condition of the rotator cuff tendons, and the degree to which conservative care has been exhausted.
Common symptoms include:
Â
Â
For overhead workers, symptoms often manifest as progressive difficulty performing job tasks â painting ceilings, wiring overhead fixtures, loading shelves â that require sustained arm elevation. For athletes, symptoms may appear as loss of velocity, endurance, or accuracy in overhead sports.
Shoulder impingement is diagnosed by an orthopedic surgeon who specializes in shoulder conditions. The evaluation typically includes:
Â
Â
Because imaging findings do not always directly correlate with symptom severity, diagnosis is based on the integration of physical examination findings, imaging, treatment history, and functional assessment.
Shoulder impingement is best evaluated and treated by an orthopedic surgeon who specializes in shoulder and sports medicine conditions. If surgery is being considered, look for a fellowship-trained shoulder surgeon â a surgeon who completed an additional year of advanced training after orthopedic residency specifically focused on shoulder conditions and procedures.
Â
Fellowship-trained shoulder surgeons have specific expertise in:
Â
Not every patient with subacromial impingement requires surgery. Conservative care â physical therapy and cortisone injections â is the appropriate first step for most patients and produces meaningful improvement in many cases.
Â
Surgery becomes appropriate when:
Â
Â
The decision to proceed with surgery is individualized. At The Joint Preservation Center, we provide a thorough evaluation and honest recommendation based on your specific imaging, treatment history, and functional goals â not a one-size-fits-all protocol.
Acromioplasty is the surgical reshaping or partial removal of the undersurface of the acromion to create more space for the rotator cuff tendons below. At The Joint Preservation Center, acromioplasty is performed arthroscopically â through small keyhole incisions using a camera and a motorized burr â without the need for an open surgical approach.
Â
During the procedure, the surgeon:
Â
Â
The procedure is performed as an outpatient (same-day) surgery under regional anesthesia. Recovery is significantly faster than rotator cuff repair because no tendon is being reattached to bone.
The terms are often used interchangeably by patients and surgeons, but technically:
Â
Â
In practice, most arthroscopic decompression procedures include both bursectomy and acromioplasty as components of the same operation. What is included depends on intraoperative findings and the specific anatomy.
Arthroscopic subacromial decompression is a well-established procedure with a high rate of patient satisfaction for appropriately selected patients â particularly those with confirmed structural impingement (hooked acromion, bone spur) who have exhausted conservative care.
Â
Success is influenced by:
Â
Â
At The Joint Preservation Center, we track outcomes for five years after surgery â not just early post-operative results â because the true measure of surgical success is whether the shoulder remains strong, pain-free, and functional over time.
Recovery after isolated arthroscopic subacromial decompression is significantly faster than after rotator cuff repair:
Â
Â
If rotator cuff repair is performed simultaneously, recovery follows the longer rotator cuff repair protocol because the tendon must heal biologically to the bone. Your surgeon will provide a specific timeline based on what was performed.
Calcific tendinitis is a distinct condition in which calcium hydroxyapatite deposits form within the rotator cuff tendons, most commonly the supraspinatus, causing pain through both direct mechanical impingement and an intense local inflammatory reaction. It can occur alongside structural impingement or independently, and its pain pattern is often different: calcific flares can be acutely severe and episodic rather than consistently activity-related. Surgical treatment through arthroscopic calcium removal is distinct from acromioplasty, though both may be performed in the same procedure when both conditions are present. Patients who have failed barbotage, shockwave therapy, or repeated cortisone injections are appropriate candidates for arthroscopic removal.Â
Cortisone injections can provide effective short-term relief for subacromial bursitis and impingement-related pain, but they address inflammation rather than the underlying structural cause. When the cause is a hooked acromion or bone spur, mechanical impingement continues between injections and the relief each injection provides tends to diminish over time. When injections are wearing off faster, providing shorter relief, or failing to produce meaningful improvement, this is a recognized clinical signal that conservative care has reached its limit. At that point, surgical decompression removes the structural cause rather than temporarily reducing its inflammatory consequence, typically providing more durable and meaningful relief.Â
Yes, and we encourage it. If you have been told you need shoulder decompression surgery and want to confirm that recommendation â or if you have been told surgery is not yet needed but your symptoms are significantly affecting your life â we offer second opinion consultations, including virtual consultations for patients who cannot travel.
Â
A second opinion from a fellowship-trained shoulder surgeon ensures that your imaging and clinical findings are being interpreted by a surgeon with specific expertise in shoulder conditions and a full understanding of the surgical options available.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
Â
If you have a PPO insurance plan with out-of-network benefits:
Â
Â
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K â $8K depending on what you need done.
Â
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-day consultations may be available
*Online visits available