
*Online Consultations Available
*Online Consultations Available

Arthroscopic Calcium Removal Surgery
Combined Decompression & Removal Surgery
Calcific + Cuff Repair Surgery
1,000+ Shoulder Surgeries performed
Rehab-Integrated

Care
Outcomes Tracked for 5 Years


Acute calcific tendonitis occurs when calcium deposits within the rotator cuff enter a spontaneous resorptive phase, triggering an intense inflammatory reaction that patients frequently describe as the worst pain they have ever experienced, appearing suddenly within hours and making any arm movement impossible. This is not a reason to wait. During the acute resorptive phase the calcium is in its most fluid and aspiratable state, meaning urgent intervention at this moment may produce the fastest and most complete resolution. Waiting often leaves residual chronic calcium and ongoing pain.
Â
Signs you may be in an acute calcific attack:
Â
What to do: Contact The Joint Preservation Center for an urgent same-day or next-day consultation. In the acute resorptive phase the window for aspiration and definitive surgical removal is limited, and acting within this window produces the most complete results.
Â
What to expect at an urgent evaluation:
Calcific tendonitis occurs when calcium hydroxyapatite deposits form within the rotator cuff tendons, most commonly the supraspinatus but also the infraspinatus and subscapularis. These deposits can remain asymptomatic for years, cause chronic aching pain, or trigger one of the most severe acute pain events in musculoskeletal medicine when they enter the resorptive phase. Your imaging findings describe the deposit across five key dimensions that directly determine surgical candidacy and the most appropriate treatment approach:
The rotator cuff consists of four tendons. The location of the calcium deposit determines pain patterns, surgical access, and the complexity of the procedure.

A. Supraspinatus (Most Common — ~80%)
The supraspinatus tendon runs along the top of the shoulder and is the most frequently involved tendon. Calcium in the supraspinatus produces pain with forward flexion, overhead reaching, and abduction — the classic calcific tendonitis pain arc between 60 and 120 degrees of arm elevation.

The infraspinatus tendon runs along the posterior shoulder. Calcium deposits in the infraspinatus produce posterior shoulder pain and pain with external rotation. Surgical access requires slight modification of the standard arthroscopic approach.

The subscapularis runs along the front of the shoulder. Anterior shoulder pain and pain with internal rotation. Less commonly involved but clinically significant when present, particularly given its proximity to the biceps tendon groove.

Least commonly involved. Posterior and inferior shoulder pain.
impinges dynamically. Surgical fixation or resection may be required.
The Gärtner classification system describes the radiographic appearance of the calcium deposit on X-ray and predicts the likelihood of spontaneous resorption vs. the need for intervention.
Dense, homogeneous, clearly outlined deposit with a well-defined border. Hard chalky consistency at surgery. Type A deposits are the least likely to spontaneously dissolve and the most likely to require mechanical intervention — shockwave, needling, or arthroscopic removal. Most surgical candidates present with Type A deposits.
Dense deposit with a defined border but a segmented internal structure. Intermediate behavior — some respond to shockwave and needling; others require surgical removal after these fail.
Inhomogeneous deposit with poorly defined borders. More likely to be in an active resorptive phase. May respond to conservative care or barbotage. However, when chronic and symptomatic, still appropriate for arthroscopic removal after failed conservative care.
Calcification at the tendon-bone interface rather than within the tendon body. Associated with tendinosis. Different pathophysiology and may require debridement or tendon repair in addition to calcium removal.
Deposit size — measured in millimeters on X-ray or ultrasound — is correlated with symptom severity and influences both conservative care response rates and surgical candidacy.
Â
Small deposits may resolve spontaneously or respond to shockwave therapy. Surgery is considered when symptoms are severe and conservative care has failed despite small deposit size.
The most common surgical size range. Medium deposits often fail shockwave therapy and barbotage — particularly Type A and B morphology. Arthroscopic removal is highly effective at this size, with complete removal achievable in the majority of cases.
Â
Large deposits are less likely to respond to shockwave or needling. Arthroscopic removal is the most reliable treatment. Large, dense deposits may fragment into multiple fragments during resorption, requiring thorough debridement at surgery.
Ultrasound characterizes the acoustic pattern of the deposit in real time — reflecting its current phase (formative, resting, resorptive) better than X-ray.
Â
Dense, clearly echogenic deposit with a strong posterior acoustic shadow on ultrasound. Hard consistency. Less likely to aspire easily with needling. Type A and B on X-ray correlation. Shockwave may attempt fragmentation; arthroscopic removal is reliable when these measures fail.
The deposit appears fluid or paste-like on ultrasound. A strong posterior acoustic shadow is reduced or absent. This is the phase associated with acute calcific attacks — the body’s inflammatory resorptive process produces intense pain. Importantly, the fluid phase makes the deposit maximally aspiratable: urgent barbotage during this window can produce dramatic relief and remove the calcium effectively. When urgent aspiration is incomplete or fails, arthroscopic removal can be performed.
Â
The deposit has partially resorbed but fragments remain. May produce ongoing symptoms. Arthroscopic debridement removes remaining fragments and associated inflammatory tissue.
Calcific tendonitis frequently coexists with other shoulder conditions that MRI identifies simultaneously — and that may be addressed in the same arthroscopic procedure.

The calcium deposit generates intense local inflammation that spreads to the subacromial bursa. Subacromial bursitis is present in most calcific tendonitis cases and contributes to impingement-like symptoms. Bursectomy is performed as part of the arthroscopic calcium removal procedure.

A structurally narrow subacromial outlet (hooked acromion, bone spur) combined with a calcium deposit creates a severe mechanical impingement pattern. When structural impingement is confirmed, subacromial decompression (acromioplasty) is performed concurrently with calcium removal.

Calcium deposits can secondarily damage the surrounding tendon, causing partial-thickness tearing. When MRI shows concurrent partial tearing, debridement of the tear margins — and in higher-grade tears, rotator cuff repair — may be performed at the same arthroscopic procedure.

Occasionally concurrent with calcific tendonitis, particularly in overhead athletes. Biceps tenodesis may be added to the arthroscopic procedure when confirmed.

*Same-day consultations may be available


X-ray confirms the presence and density of the deposit, ultrasound characterizes its current phase and real-time aspiratability, and MRI assesses concurrent soft tissue pathology including bursitis, cuff integrity, and biceps involvement. Imaging must be interpreted alongside symptom duration, pain severity, prior treatment history, and functional demands to determine the most appropriate next step. A shoulder specialist integrates all of these factors before determining whether urgent aspiration, elective shockwave, or arthroscopic calcium removal is indicated and whether concurrent procedures are needed.Â

Calcific tendonitis does have a natural history of spontaneous resorption in some patients, which is why initial conservative management is appropriate before surgical evaluation. However, resolution is unpredictable, may take 1 to 3 years, and is far from guaranteed. Type C deposits are most likely to resorb spontaneously, while Type A and B deposits are significantly less likely to resolve without intervention. Once shockwave therapy has failed to fragment the deposit and ultrasound-guided barbotage has failed to aspirate it, waiting for natural resolution is no longer a reasonable strategy. The deposit has demonstrated it will not dissolve on its own, and arthroscopic removal definitively addresses what conservative care cannot.Â

Daily activity:
Â
Athletic and sport impact:
Â
Occupational impact:
Calcific tendonitis follows a more defined treatment pathway than almost any other shoulder condition before surgery becomes appropriate:
Â
Â
Shockwave therapy resolves calcific tendonitis in approximately 50 to 70% of patients, and barbotage resolves it in a further subset. For patients with Type A dense deposits, large deposits, or deposits that do not respond to these measures, arthroscopic calcium removal is the definitive solution.

Conservative and intermediate care CAN:
Â
Conservative and intermediate care CANNOT:

Treatment selection depends on deposit type (Gärtner classification), deposit size, deposit phase (hard vs. resorptive), symptom duration, prior treatment history, concurrent pathology, and the patient’s functional demands and timeline. A stepwise approach is appropriate — moving to arthroscopic removal when the intermediate steps have failed.
For patients who have not yet completed the conservative and intermediate procedure pathway, these treatments are appropriate first steps:
Â
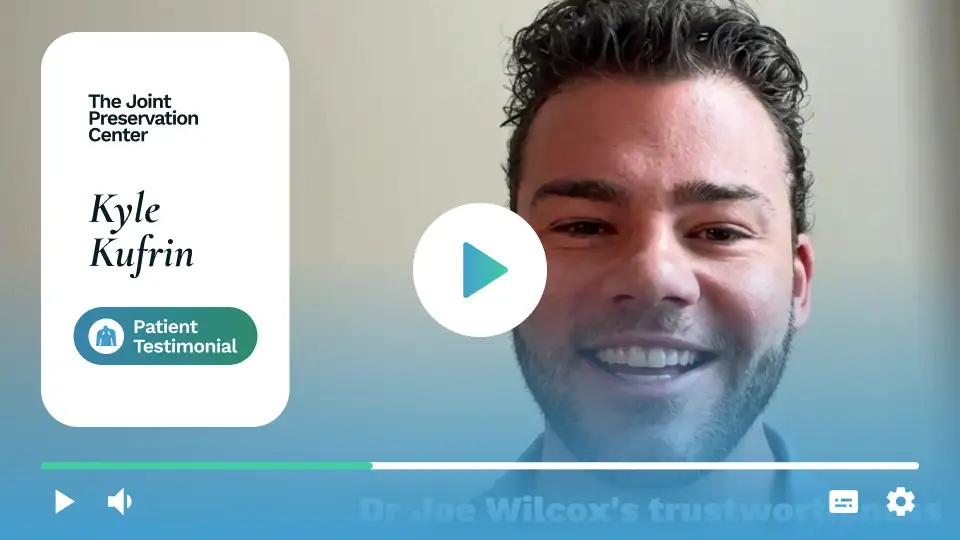
Arthroscopic calcium removal is the definitive surgical treatment for calcific tendonitis that has failed conservative and intermediate management. The procedure directly visualizes and removes the calcium deposit under arthroscopic guidance, achieving complete and verified removal under direct vision while simultaneously addressing all concurrent pathology. It is associated with very high success rates, particularly for Type A and B deposits resistant to conservative measures, and most patients experience dramatic and durable pain relief.Â
Arthroscopic calcium removal is performed as an outpatient procedure under regional anesthesia with sedation or general anesthesia, typically taking 30 to 60 minutes for isolated calcium removal and longer when combined with concurrent procedures.
Â
During the procedure:
Â
Â
The key advantage over barbotage is direct visualization, allowing the surgeon to confirm complete removal rather than relying on the indirect feel of aspiration.

The goal of arthroscopic calcium removal is complete removal of the accessible deposit, and in most cases substantial to complete removal is achieved under direct visualization. Small amounts of calcium occasionally remain at the tendon-bone interface or within dense ossified deposits, which is why the calcified material is incised and irrigated thoroughly. Studies show that even partial removal produces excellent clinical outcomes, as the remaining calcium does not regenerate the intense inflammatory response associated with the intact deposit, and patient satisfaction is high regardless of whether radiographic removal is complete or near-complete.Â
Sling
Typically 5–10 days for comfort, depending on whether concurrent procedures (cuff repair, decompression) were performed. Isolated calcium removal has minimal sling requirements — the tendon is not reattached to bone.
Â
Return to Desk Work
Often within 1–2 weeks.
Â
Return to Overhead Work (Construction, Painting, Electrical)
Typically 6–10 weeks for isolated calcium removal. Longer if concurrent decompression or cuff repair was performed.
Â
Return to Swimming
Freestyle and overhead strokes typically at 8–12 weeks. Competitive return at 3–4 months.
Â
Return to Overhead Sport (Pitching, Volleyball, Tennis)
Interval throwing typically begins at 8–10 weeks. Full competitive return at 3–5 months depending on sport and concurrent procedures.
Â
Return to CrossFit Overhead Movements
Kipping pull-ups and loaded overhead at approximately 10–14 weeks.
Â
Recovery is significantly faster than rotator cuff repair because no tendon reattachment is required. The primary recovery driver is resolution of post-surgical inflammation and progressive restoration of shoulder strength through rehabilitation.


Calcific tendonitis rarely occurs in isolation from other shoulder pathology. MRI frequently identifies concurrent bursitis, subacromial impingement, and rotator cuff involvement that requires simultaneous surgical attention. At The Joint Preservation Center, we address all relevant pathology in a single arthroscopic procedure where possible — eliminating the need for multiple surgeries.
The most common combined procedure. Subacromial impingement — from a hooked acromion or bone spur — mechanically compresses the calcium-bearing tendon with every arm movement, amplifying pain and inflammation. When structural impingement is confirmed on X-ray and MRI, arthroscopic decompression is performed at the same time as calcium removal: acromioplasty reshapes the acromion to create adequate subacromial space, and bursectomy removes the chronically inflamed bursa.
Â
Combined calcium removal and decompression does not meaningfully extend recovery beyond isolated calcium removal alone.
When MRI shows concurrent partial-thickness rotator cuff tearing alongside the calcium deposit — which occurs when chronic calcium inflammation has damaged the surrounding tendon — the tearing is addressed at the same arthroscopic procedure.
Â

Calcific tendonitis occasionally affects both shoulders simultaneously, or the second shoulder develops calcium deposits after the first is treated. Bilateral involvement is managed sequentially — one shoulder addressed first, the second after adequate recovery — to minimize cumulative functional limitation.

Modern arthroscopic stabilization techniques are associated with:
High rates of re-dislocation prevention
Significant gains in shoulder confidence and function
Improved functional outcome scores
High patient satisfaction
1
We evaluate your symptoms, shoulder strength and movement, review your X-ray, ultrasound, and MRI, and discuss your treatment history — including prior shockwave sessions, barbotage attempts, and injection history. For acute attack patients, we provide urgent same-day evaluation with immediate aspiration if the deposit is in the fluid/resorptive phase.
2
We explain whether additional conservative steps remain appropriate — or whether arthroscopic calcium removal is the most appropriate next step based on your deposit type, treatment history, and functional goals. For patients who have failed shockwave and barbotage, the answer is almost always surgical.
3
If surgery is recommended, our fellowship-trained shoulder surgeons perform arthroscopic calcium removal — with any concurrent indicated procedures (decompression, bursectomy, cuff repair) — through small keyhole incisions to definitively eliminate the structural pain source.
4
Our surgeons work closely with physical therapists to guide a progressive rehabilitation program — restoring motion, rebuilding strength, and progressing sport-specific or occupation-specific loading as the shoulder heals.
5
Rehabilitation progresses through milestones so you can confidently return to swimming, throwing, overhead work, and the activities that calcific tendonitis has been preventing — without the constant pain that has defined the condition.
This long-term follow-up helps us understand how patients recover beyond the early healing period — including pain resolution, return to heavy pressing, return to overhead occupational work, and long-term AC joint stability. These insights allow our surgeons to continually refine surgical planning and rehabilitation protocols to support durable shoulder performance over time.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
Calcific tendonitis is the formation of calcium hydroxyapatite deposits within the rotator cuff tendons, most commonly the supraspinatus. These deposits can remain asymptomatic, cause chronic aching shoulder pain, or trigger an acute calcific attack during the resorptive phase, one of the most intense acute pain events in musculoskeletal medicine. The condition progresses through a formative phase where calcium accumulates quietly, a resting phase where the deposit stabilizes, and a resorptive phase where the body attempts to dissolve the deposit and triggers intense inflammation. Surgery is most commonly performed for deposits that have failed to resolve during the resorptive phase or for Type A dense deposits resistant to conservative and intermediate treatment.Â
Symptoms vary dramatically based on the phase:
Â
Chronic phase (most common):
Â
Acute resorptive phase:
Extracorporeal shockwave therapy (ESWT) uses high-energy acoustic waves directed at the calcium deposit to fragment and dissolve it, with resolution rates of approximately 50 to 70% across multiple studies. However, it fails in a significant proportion of patients, primarily those with Type A dense deposits that are resistant to fragmentation, as acoustic waves cannot effectively penetrate a very hard homogeneous calcium mass. Multiple sessions are typically recommended before concluding that ESWT has failed. When shockwave therapy has not produced deposit reduction after an adequate course of treatment, arthroscopic calcium removal is the appropriate next step rather than additional shockwave sessions.
Barbotage (ultrasound-guided needling and lavage) is a procedure in which a needle is directed into the calcium deposit under ultrasound guidance, and the calcium material is aspirated and lavaged (washed out). It is most effective when the calcium is in the fluid/paste resorptive phase — in this state, the calcium can be drawn out through the needle.
Â
Barbotage fails — as it often does with Type A dense deposits — when the calcium is hard and chalk-like rather than fluid. The needle cannot aspirate solid calcium material. Failed barbotage is one of the clearest signals of surgical candidacy: the deposit is physically resistant to non-surgical removal, and arthroscopic removal under direct visualization is the only remaining option that definitively addresses the problem.
For patients who have not yet tried shockwave therapy, ESWT is the appropriate first step, being non-invasive and effective in approximately 50 to 70% of patients. For patients whose shockwave therapy has failed, or who have also failed barbotage, arthroscopic calcium removal is consistently superior in evidence-based comparisons, with higher resolution rates, faster return to function, and higher patient satisfaction. The decision is not surgery versus shockwave but rather surgery versus continued waiting after shockwave has already failed, and for that specific group surgery is the clearly superior choice.Â
Calcium recurrence after arthroscopic removal is uncommon — substantially lower than after shockwave therapy alone. The direct, mechanically complete removal of the deposit under arthroscopic visualization removes the calcium at its source, rather than attempting to dissolve it indirectly.
Â
Studies report calcium recurrence rates of approximately 5–15% after arthroscopic removal at long-term follow-up — compared to higher rates after shockwave therapy alone. Even in cases of partial recurrence, the residual deposit is typically smaller, less dense, and less symptomatic than the original.
Arthroscopic calcium removal is associated with very high success rates for appropriately selected patients — patients who have failed conservative and intermediate measures. Published studies report patient satisfaction rates of 80–95%, with most patients experiencing durable pain relief and return to previous activity levels.
Â
Success is highest when: the deposit is confirmed by imaging, surgery is performed after adequate conservative care has been exhausted, concurrent pathology (impingement, bursitis) is addressed at the same procedure, and the patient completes the prescribed rehabilitation program.
Recovery after isolated arthroscopic calcium removal is significantly faster than after rotator cuff repair:
Â
If concurrent rotator cuff repair was performed, recovery follows the longer rotator cuff repair timeline. Your surgeon will provide specific guidance based on what was performed.
Yes, and we encourage it — particularly if you have been told to keep trying shockwave therapy after it has already failed multiple times, or if you have been told surgery is not an option. We offer second opinion consultations, including virtual consultations for patients who cannot travel.
Â
A second opinion from a fellowship-trained shoulder surgeon confirms whether your treatment history genuinely indicates surgical candidacy — and whether arthroscopic calcium removal is the most appropriate next step for your specific deposit type, size, and history.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
Â
If you have a PPO insurance plan with out-of-network benefits:
Â
Â
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K – $8K depending on what you need done.
Â
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-day consultations may be available
*Online visits available