*Online Consultations Available

*Online Consultations Available
1,000+ Shoulder Surgeries performed
Rehab-IntegratedâĻ
Care
Outcomes Tracked for 5 Years


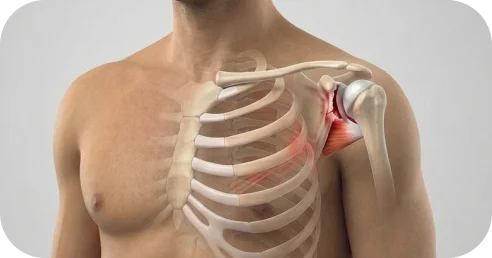
A Bankart tear means that the labrum â the cartilage ring that deepens the shoulder socket and anchors the ligaments that prevent dislocation â has torn away from the front of the glenoid, leaving the shoulder structurally vulnerable to coming out of the socket.
Â
MRI reports can describe a Bankart tear across six factors:
The labrum can detach in several distinct patterns, and MRI may show one or more structural injuries.





This refers to the degree of glenoid bone erosion â measured on CT with 3D reconstruction. It is one of the most critical factors in surgical planning.

This refers to the measured extent of labral detachment around the glenoid clock face.
Â

This refers to how and when the shoulder became unstable.
Â

Displacement describes how far the torn labrum has moved from its original attachment on the glenoid rim.
Â

This refers to the condition of the labral tissue and surrounding structures. Tissue quality influences healing potential, repair complexity, and long-term stability.



If labral tissue quality is significantly compromised, bone augmentation â the Latarjet procedure â may provide more reliable long-term stability than soft tissue repair alone.

*Same-day consultations may be available


Even though an MRI and CT provide valuable structural information, they do not establish a complete diagnosis. A Bankart tear must be interpreted in the context of dislocation history, shoulder function, apprehension patterns, and the physical demands placed on your shoulder â both now and over time.
Â
A shoulder specialist integrates these factors through comprehensive evaluation before defining the most appropriate path forward.

Natural healing is unlikely.
Â
When the labrum detaches from the glenoid rim, the fibrocartilage loses its blood supply and structural contact with bone â much like a rubber band that has snapped free of its anchor. Without proper treatment, the torn tissue does not predictably reattach, and the shoulder remains structurally vulnerable to re-dislocation.
Â
A comprehensive evaluation by a shoulder specialist can help determine the best path forward.
Bankart tears vary in behavior. Some patients function with manageable instability for a period; others experience rapid escalation.
Â
Risk of progression increases with each subsequent dislocation â as bone is lost from the front of the socket, the force required to dislocate decreases, and the structural reconstruction required becomes significantly more complex.

When instability is left untreated, structural changes develop:
Â
Â
These changes may translate into functional limitations:
Â
In daily lifeâĻ
Â
Â
Sports & performanceâĻ
Â
Â
As bone loss accumulates and instability worsens, the reconstruction required becomes more complex and the probability of full return to sport decreases.


Appropriate treatment for a Bankart tear depends on multiple factors, including the type and extent of labral injury, the degree of bone loss, the number of prior dislocations, activity demands, and short- and long-term goals.
For some patients â particularly first-time dislocators who are older, lower-activity, or not engaged in contact sports â structured physical therapy may be appropriate as an initial management approach. It is important, however, to understand what therapy can and cannot accomplish.
A well-designed rehabilitation program can:
Â
Â
Some patients experience meaningful improvement within 6â12 weeks when therapy is structured and progressive.


Physical therapy alone may be less appropriate when:
Â
Â
For working adults and athletes, the decision to move beyond therapy is often practical: the shoulder is no longer meeting the demands of work, training, or daily activity. If instability recurs after a structured program, this reflects the structural limits of conservative care â and may indicate that surgical stabilization is needed to restore reliable function.

A comprehensive evaluation can determine whether structured rehabilitation is appropriate for your specific situation â and what type of program is most likely to be effective.
When a Bankart tear causes recurrent instability, involves significant bone loss, or has failed conservative management, surgical repair may be necessary to reestablish proper shoulder mechanics.
Arthroscopic Bankart repair reattaches the torn labrum and its attached stabilizing ligament back to the front of the shoulder socket.
Â
If the labrum is fully detached, it is mobilized and secured back to its original attachment on the glenoid rim.
Â
If the capsule is lax or a rotator interval defect is present, the appropriate tightening procedure is performed alongside the repair.

When the labrum reattaches to the glenoid rim:
Â
Â
For most patients, successful repair results in:
Â
Â
Outcomes depend on the type of labral injury, bone loss, timing of repair, structured rehabilitation, and the surgeon’s experience in managing Bankart tears.

Bankart repair is performed arthroscopically through small incisions using a specialized camera to visualize the shoulder.
Â
The procedure is typically done under regional anesthesia with sedation or general anesthesia.
Â
During surgery, the surgeon:
Â
Small anchors â typically biocomposite or titanium â are placed into the prepared glenoid rim at the labrum’s original attachment site. Strong sutures threaded through these anchors secure the labrum back to the bone under controlled tension, restoring the cartilage bumper effect and the ligamentous restraint against dislocation.
Â
At The Joint Preservation Center, the number and configuration of anchors is selected based on the extent and pattern of labral detachment.
Â
Incisions are typically only a few millimeters in size. Because the procedure is performed through small incisions using a camera and specialized instruments â sometimes called keyhole surgery â tissue disruption is minimized, which supports faster early recovery compared to open approaches.
Â
The procedure generally takes one to one and a half hours, depending on complexity. Healing occurs gradually over several months as the labrum integrates into the glenoid bone.

Pain and Early Recovery After Surgery
Â
Most patients experience moderate discomfort in the first several days, managed with a combination of regional anesthesia, oral medication, and icing.
Â
A sling is worn to protect the repair, typically for 4â6 weeks depending on the extent of labral injury. The purpose of the sling is to prevent early strain on the healing labrum.
Â
Pain typically improves steadily over the first 1â2 weeks.
Â
Sleeping is often most comfortable in a slightly upright position during the early phase.

Bankart repair heals in phases. Although the labrum is secured during surgery, biological integration to the glenoid bone takes time â and protection during early recovery is essential.
Â
Recovery progresses in structured stages:
Â
Phase 1: Protection and Passive Motion (Weeks 0â4/6)
Gentle guided movement begins early to prevent stiffness while protecting the repair. The repaired labrum is not yet structurally strong.
Â
Phase 2: Active Motion (Weeks 4/6â8/10)
You begin moving the shoulder under your own power as healing progresses.
Â
Phase 3: Strengthening (After ~10â12 Weeks)
Controlled strengthening begins once the labrum has biologically started to integrate into the bone. Rotator cuff and scapular stabilizer strength are rebuilt gradually.

Drive?
Usually when you are out of the sling and off narcotic pain medication â typically 4â6 weeks.
Â
Return to desk work?
Often within 1â2 weeks, depending on comfort.
Â
Return to manual labor?
Typically 3â4 months, depending on demands.
Â
Return to sports?
Non-contact activities may resume gradually around 4â5 months. Contact and collision sports â football, wrestling, rugby, MMA â typically require 5â6 months based on objective strength milestones, not time alone.
Â
Timelines vary based on the extent of labral injury, bone loss, and healing response. Full shoulder confidence can continue improving for up to a year.
Successful recovery depends on:
Â
Evidence shows that untreated shoulder instability can:
Â
Â
These structural changes may reduce the effectiveness of surgery and increase repair complexity later.
Â
This does not mean every Bankart tear requires immediate surgery. It does mean that appropriate timing matters when structural compromise is progressing.

One of the most common concerns for working adults considering Bankart repair is timing: how to schedule the procedure around professional obligations, minimize income disruption, and plan for the weeks when full function is not yet restored.
Â
Desk work and computer-based roles: Most patients return to desk work within 1â2 weeks, working one-handed or with limited arm use initially. Typing with both hands is generally comfortable within 3â4 weeks.
Â
Supervisory, managerial, or client-facing roles: If your work does not require physical lifting, return within 1â2 weeks is typical. Driving is usually possible once the sling is discontinued and you are off narcotic medication, generally within 4â6 weeks.
Â
Manual labor, construction, trades, or physical occupations: Return to light duty may be possible within 2â3 months. Return to full overhead or heavy lifting duties typically requires 4â6 months. Some employers offer modified duty during this transition.
Â
Work restrictions documentation: We provide work restriction letters and return-to-work clearance documentation as needed for your employer or occupational health department.
Return-to-sport timelines depend on the demands of your activity, the complexity of your repair, and your progress through rehabilitation milestones.
These timelines are approximations. Your specific return-to-sport plan is developed collaboratively between your surgeon and your physical therapist based on objective strength milestones.
Preparing your home and support system before surgery helps the early recovery period go more smoothly. Because you will be in a sling and restricted from using your operative arm for several weeks, some advance planning makes a meaningful difference:
Â
Â
Patients who plan ahead consistently report a smoother, less stressful early recovery.
Recovery after Bankart repair can vary depending on the extent of labral injury, the degree of bone loss, and the specific procedure performed.
Â
While general timelines can be helpful for orientation, your recovery plan will be personalized. Your surgeon will guide you through a protocol tailored to your shoulder, your goals, and your lifestyle.
Week 1: Sling at all times. Pain management with medication, icing, and rest. Begin gentle pendulum exercises as directed. Most discomfort resolves significantly by day 5â7.
Â
Weeks 2â3: First postoperative visit. Passive range-of-motion exercises with a therapist begin. Pain continues to improve. Desk work may resume if comfortable.
Â
Weeks 4â6: Gradual progression of passive and assisted motion. Sling is typically discontinued. Driving may resume once the sling is off and narcotic medication is no longer needed.
Â
Weeks 6â10: Transition from passive to active motion. The shoulder begins moving under its own power. Daily activities become noticeably easier.
Â
Weeks 10â16: Strengthening begins. Rotator cuff and scapular stabilizer exercises rebuild shoulder strength and neuromuscular control.
Â
Months 4â5: Progressive sport-specific or job-specific rehabilitation. Non-contact sport return for eligible patients.
Â
Months 5â6: Contact sport return criteria assessment â strength and functional testing. Full contact clearance for most athletes.
Â
Months 6â12: Continued strength gains. Full confidence with high-demand activities. Strength can continue improving for up to a year after surgery.

Not every Bankart tear can be addressed with a straightforward arthroscopic repair. Significant bone loss, engaging Hill-Sachs defects, complex lesion variants, combined shoulder pathology, and failed prior repairs each present distinct surgical challenges that require advanced techniques and specialized experience.
Â
At The Joint Preservation Center, we evaluate the full spectrum of shoulder instability pathology and offer the appropriate procedure for your specific anatomy â rather than a one-size-fits-all approach.
When glenoid bone loss exceeds the threshold at which soft tissue repair alone is unreliable â typically 20â25% of the glenoid surface area â the Latarjet procedure offers a bone reconstruction solution that addresses both the missing bone and the dynamic stability deficit.
Â
The Latarjet transfers the coracoid bone â a natural projection at the front of the shoulder blade â along with its attached conjoined tendon to the deficient anterior glenoid. This achieves two stabilizing effects: the bone graft restores the missing glenoid arc, and the conjoined tendon creates a dynamic sling that tightens when the arm is in the vulnerable abducted-externally-rotated position.
Â
Who Is a Candidate for the Latarjet Procedure?
Â
The Latarjet may be appropriate for patients with glenoid bone loss exceeding approximately 20â25%, an inverted pear glenoid shape on CT, a failed prior arthroscopic Bankart repair, or a high-demand contact sport athlete with subcritical bone loss and an engaging Hill-Sachs defect.
Â
Latarjet Recovery for Active Adults
Â
Sling immobilization is typically 4â6 weeks, with passive motion beginning in the early postoperative period. Active strengthening begins around weeks 10â12 after bone graft healing is confirmed on imaging. Return to contact sport typically requires 6â9 months with CT confirmation of graft incorporation before clearance.
When a Hill-Sachs defect on the back of the humeral head is ‘engaging’ â locking over the glenoid rim during movement and predisposing to re-dislocation even after labral repair â remplissage can address this humeral-side contribution to instability.
Â
Remplissage fills the Hill-Sachs defect by arthroscopically suturing the posterior capsule and infraspinatus tendon into the bony cavity, converting the engaging pattern into a non-engaging one. The procedure is performed during the same operation as Bankart repair, adding approximately 20â30 minutes.
Â
Who Is a Candidate for Remplissage?
Â
Remplissage may be appropriate when glenoid bone loss is below the Latarjet threshold, the Hill-Sachs lesion is engaging on CT assessment, and the combined arthroscopic approach can address both labral and humeral-head pathology in a single operation. For overhead throwing athletes, the decision between remplissage and Latarjet requires individualized analysis, as remplissage may modestly reduce end-range external rotation.
Â
RecoveryâĻ
Â
Recovery following combined Bankart repair with remplissage follows a similar phased protocol to standard Bankart repair. The sling duration and return-to-sport timelines are comparable, adjusted for the complexity of the combined procedure.

Many Bankart tears do not occur in isolation. Imaging frequently reveals concurrent pathology â a SLAP tear alongside a Bankart, rotator cuff involvement with anterior instability, or a Hill-Sachs defect requiring remplissage. When multiple structures are compromised, addressing only the Bankart may leave residual symptoms.

Bankart Repair with SLAP Repair
A SLAP tear involves the superior labrum â the cartilage at the top of the shoulder socket where the biceps tendon anchors. In overhead athletes and patients with traumatic shoulder injuries, a SLAP tear may coexist with a Bankart tear. When both structures are compromised, addressing the anterior labrum alone may leave superior labral instability or biceps anchor pain. We evaluate each case to determine whether the SLAP requires repair, debridement, or biceps tenodesis, and perform the appropriate combined procedure to restore both anterior and superior labral stability.

Bankart Repair with Rotator Cuff Repair
Â
Anterior shoulder instability can involve subscapularis pathology â particularly in patients with combined injury patterns or high-energy dislocations. When rotator cuff involvement is identified on imaging or intraoperatively, the appropriate combined procedure addresses both cuff integrity and labral stability in a single operation.
Some patients present with shoulder instability in both shoulders. Bilateral involvement is particularly common in patients with underlying capsular laxity or after contact sport careers with dislocation events on both sides.
Â
Bilateral surgery is typically staged â one shoulder is stabilized first, and the second is addressed after the first has recovered sufficiently to manage daily activities. We develop a surgical and rehabilitation plan that sequences bilateral procedures to minimize cumulative downtime, which is especially important for working adults managing career obligations and caregiving responsibilities.

A Bankart repair that does not hold â whether due to missed bone loss, anchor failure, a new traumatic event, or biological failure â leaves patients with persistent instability after already making the recovery investment. For working adults and athletes, a failed primary repair is especially disruptive.
Â
When Is Revision Surgery Appropriate?
Â
Revision stabilization may be considered when imaging confirms structural failure of the primary repair, instability has not resolved after adequate postoperative rehabilitation, and the remaining anatomy supports a revision procedure. At The Joint Preservation Center, we evaluate revision cases with MRI arthrogram and CT 3D reconstruction to assess current bone loss â which may have increased since the primary surgery â and to determine what contributed to the initial failure.
Â
Signs of Repair Failure to Watch For
Â
Patients should be aware of potential signs that a repair may not be holding: a sudden return of apprehension or dislocation after an initial period of improvement, inability to progress through rehabilitation milestones, a specific re-injury event with immediate loss of stability, or recurrent dislocation in the months after primary repair. Any of these warrant reevaluation.
Â
Revision ApproachesâĻ
Â
Depending on the revision scenario, we may convert to the Latarjet procedure â the most common revision pathway after failed arthroscopic Bankart repair â perform revision arthroscopic repair in select cases with specific technical failure, use glenoid bone grafting (Eden-Hybinette or distal tibial allograft) for massive bone loss, or perform capsular reconstruction where capsular insufficiency is a primary contributing factor. The revision plan is determined by what the anatomy and biology can support at the time of reevaluation.
Chronic instability arthropathy is a distinct condition that can develop when longstanding, recurrent shoulder instability leads to progressive glenoid bone erosion and eventual joint deterioration. Over time, the cumulative loss of the glenoid’s anterior rim â combined with repeated episodes of cartilage impact â can cause abnormal wear patterns and structural joint changes. This is not simply a large bone loss case â it represents a progressive transformation of the glenoid that requires a different reconstruction approach.
Â
When Glenoid Reconstruction Is the Right Option
Â
For patients with established massive glenoid bone deficiency â where the defect exceeds what the Latarjet coracoid transfer can reliably address, or where the coracoid is unavailable due to prior harvest â glenoid reconstruction with distal tibial allograft (DTA) or iliac crest autograft may be the most appropriate path to restoring a stable, functional shoulder socket. DTA closely approximates the natural glenoid curvature and is secured with screws, restoring the glenoid arc.
Â
At The Joint Preservation Center, our approach is to exhaust all standard reconstruction options before proceeding to complex bone grafting. Glenoid reconstruction is reserved for situations where the available bone stock cannot support a simpler stabilization procedure.
Â
For working-age patients and athletes, this decision carries particular weight. Graft healing timelines, activity progression, and long-term durability are discussed in detail so you can make a fully informed decision about your shoulder’s trajectory.


Modern arthroscopic stabilization techniques are associated with:
High rates of pain improvement
Significant gains in shoulder confidence and function
Improved functional outcome scores
High patient satisfaction
1
We evaluate your symptoms, shoulder stability, strength and movement, review your imaging â including MRI arthrogram and CT bone loss measurements â and consider your dislocation history, goals, and lifestyle. If additional imaging is needed, it can be ordered.
2
We explain whether rehabilitation or surgical stabilization is appropriate based on your labral injury, bone loss, instability pattern, and goals.
3
If surgery is recommended, our fellowship-trained shoulder surgeons perform the appropriate stabilization procedure â arthroscopic Bankart repair, Latarjet coracoid transfer, remplissage, or revision stabilization â to restore shoulder stability and prevent further dislocation.
4
Our surgeons work closely with physical therapists to guide a structured rehabilitation program that restores motion and strength while protecting the repair.
5
Rehabilitation progresses through milestones so you can confidently return to the activities that matter most â work, exercise, and sport.
This long-term follow-up helps us understand how shoulders recover beyond the early healing period â including re-dislocation rates, return to sport, functional strength, and patient satisfaction. These insights allow our surgeons to continually refine surgical planning and rehabilitation strategies to support durable shoulder stability over time.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
The shoulder labrum is a ring of fibrocartilage that surrounds and deepens the shoulder socket (glenoid).
Â
The labrum works to:
Â
Â
A Bankart tear is a detachment of the anterior-inferior labrum â the segment at the front and bottom of the socket â from the glenoid rim. When this anchor tears away, the shoulder loses its primary structural defense against dislocation and is predisposed to re-dislocation with overhead and external rotation movements.
Bankart tears and shoulder instability can cause several symptoms depending on the severity and chronicity of the injury.
Â
Common symptoms include:
Â
Â
Some patients experience progressive instability with worsening over time; others notice sudden onset after a specific traumatic event.
Bankart tears are typically diagnosed by an orthopedic surgeon who specializes in shoulder instability conditions.
Â
During evaluation, the surgeon reviews your dislocation history and performs a physical examination that includes specific instability tests â the apprehension test, relocation test, and anterior load and shift.
Â
Imaging studies are then used to confirm the diagnosis and better understand the structural injury:
Â
Â
Because imaging findings must be interpreted alongside clinical history and functional examination, the final diagnosis is based on a combination of all three.
Bankart tears and shoulder instability are treated by orthopedic surgeons who specialize in shoulder and sports medicine conditions.
Â
For the highest level of specialization, look for a fellowship-trained shoulder surgeon. Fellowship training is an additional year of advanced surgical training completed after orthopedic residency. During this period, surgeons focus specifically on complex shoulder instability conditions and procedures.
Â
This training typically includes:
Â
Â
Fellowship-trained shoulder surgeons often have deeper experience in the full spectrum of instability procedures â from soft tissue repair to complex bone reconstruction â which matters most in cases involving bone loss, engaging Hill-Sachs, or prior failed surgery.
Patients do not feel pain during Bankart repair. The procedure is typically performed under regional anesthesia with sedation or general anesthesia, so the shoulder is completely numb during the operation.
Â
After surgery, some discomfort is expected â particularly during the first 48â72 hours, when the initial inflammatory response is strongest. Pain is usually managed effectively with a combination of medication, ice, sling support, and activity modification.
Â
Many patients also receive a regional nerve block, which can keep the shoulder numb for several hours after surgery and help make the first day significantly more comfortable.
Â
Sleeping can feel awkward at first because the shoulder must be protected in a sling. Many patients find it more comfortable to sleep slightly upright or supported with pillows during the first couple of weeks.
Â
As healing progresses, pain typically improves steadily. Structured rehabilitation then helps restore motion and strength while protecting the repair.
For most patients, the short-term recovery period is worthwhile because successful stabilization eliminates the fear of dislocation, restores shoulder confidence, and allows return to sport and work.
Arthroscopic Bankart repair is a reliable procedure for appropriately selected patients, especially when bone loss is minimal, tissue quality is adequate, and rehabilitation is followed closely.
Â
Outcomes vary with:
Â
Â
In general, patients with minimal bone loss and soft tissue Bankart lesions achieve low re-dislocation rates â approximately 5â10% at 2-year follow-up. In bone loss cases requiring the Latarjet procedure, re-dislocation rates are below approximately 4% at long-term follow-up.
Â
From the patient’s perspective, success is usually measured by more than re-dislocation rates alone. Most patients want to know whether apprehension resolves, sport participation is restored, and the shoulder is reliable again for work and daily life.
Â
At The Joint Preservation Center, our surgeons track outcomes for 5 years because durable shoulder stability â not just early pain relief â is the true measure of success.
Recovery after Bankart repair occurs in phases because the labrum must heal back to the glenoid bone.
Â
Most patients wear a sling for 4â6 weeks to protect the repair while early healing takes place. During this time, gentle guided motion is introduced to keep the shoulder mobile without stressing the repair.
Â
Over the following weeks, rehabilitation gradually progresses to strengthening as the labrum continues to heal.
Â
Many patients regain meaningful day-to-day function within 3â4 months. Full confidence with contact sport, overhead activity, and high-demand physical work typically requires 5â6 months for Bankart repair and 6â9 months for Latarjet.
Â
A structured rehabilitation program and adherence to recovery guidelines play an important role in achieving the best possible outcome.
Unlike Bankart repair â which restores native tissue and preserves the natural shoulder joint â shoulder replacement involves implanting metal and polyethylene components. Replacement is not a treatment for shoulder instability or Bankart tears.
Â
Â
Shoulder replacement is relevant only in very specific end-stage scenarios â such as glenohumeral arthritis developing after decades of untreated instability, which is precisely the outcome that early Bankart repair aims to prevent.
Yes, many patients continue to use their shoulder with a known Bankart tear, particularly in the early or less-severe stages of instability.
Â
Other muscles around the shoulder can temporarily compensate for the structural deficiency, allowing the arm to move. However, this compensation often comes with apprehension, reduced confidence, or avoidance of the positions that previously caused dislocation.
Â
Over time, continued instability may lead to worsening bone loss, increasing capsular laxity, and eventual loss of functional capacity â which is why evaluation and treatment planning are important even when function feels manageable in the short term.
Bankart tears can occur either suddenly from a traumatic event or, in some overhead athletes, through repetitive stress on the shoulder.
Â
Traumatic dislocations are the most common cause â a fall, collision, tackle, or forceful arm movement that drives the humeral head forward and out of the socket. Patients typically notice immediate pain, instability, and the need for reduction. A single high-energy dislocation can produce a complete Bankart lesion.
Â
Recurrent instability develops when a first dislocation is not definitively treated and subsequent events occur. Each repeat dislocation adds structural damage â more bone loss, a deeper Hill-Sachs, and greater capsular laxity.
Â
Both patterns can result in progressive shoulder instability that limits sport, work, and daily activity.
Chronic shoulder instability refers to a persistent pattern of repeated dislocation or subluxation â where the shoulder cannot reliably maintain its position in the socket despite conservative treatment. It develops when the initial structural injury is not definitively addressed, and cumulative bone loss, capsular laxity, and labral degeneration compound over time.
Â
Chronic shoulder instability is an important clinical finding because it typically indicates advanced structural compromise â including significant bone loss, ALPSA scarring, capsular laxity, and potentially engaging Hill-Sachs â that may require complex reconstruction rather than straightforward arthroscopic repair. If you are experiencing repeated dislocation episodes or persistent apprehension with shoulder use, evaluation by a shoulder specialist experienced in complex instability management is recommended.
Yes. It is common for MRI arthrogram to reveal concurrent pathology alongside a Bankart tear â including Hill-Sachs lesions requiring remplissage, SLAP tears (superior labral tears), HAGL lesions on the humeral side, rotator cuff pathology, or significant glenoid bone loss requiring augmentation.
Â
We routinely address combined shoulder pathology during a single procedure. For example, Bankart repair can be combined with remplissage, SLAP repair, Latarjet bone augmentation, or rotator cuff repair depending on what your imaging and intraoperative findings indicate. Addressing all contributing structures in one operation avoids the need for a second surgery and typically produces better overall outcomes.
Bilateral shoulder instability is managed with a staged approach â one shoulder is stabilized first, and the second is addressed after the first has recovered sufficiently to manage daily activities comfortably. We develop a sequencing plan that minimizes total downtime, which is especially important for patients managing work obligations and family responsibilities.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
Â
If you have a PPO insurance plan with out-of-network benefits:
Â
Â
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K â $8K depending on what you need done.
Â
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-day consultations may be available
*Online Consultations Available