
1,000+ Shoulder Surgeries performed
Rehab-Integrated

Care
Outcomes Tracked for 5 Years
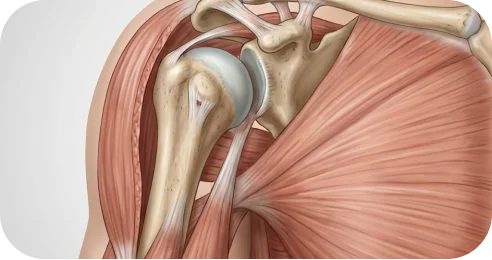
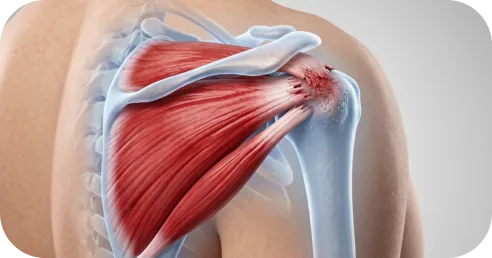
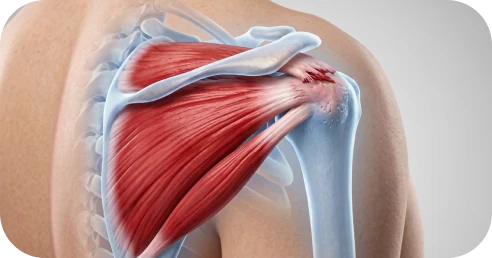
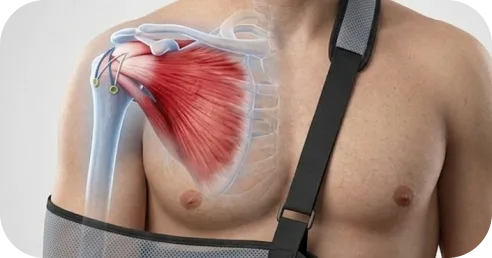
A rotator cuff tear means that one of the four shoulder tendons — the structures that attach muscle to bone and help lift and stabilize the arm — has partially or completely separated from the bone.

MRI reports can describe a rotator cuff tear across six factors:
The rotator cuff consists of four tendons, and an MRI may show that one or more are torn.

A. Supraspinatus tear



This refers to the measured width of the tear.
Â

This refers to how and when the tear occurred.
Â
Retraction describes how far the torn tendon has moved away from its normal attachment site. Applies primarily to full-thickness tears.
Â

This refers to the health of the tendon and surrounding muscle. Tissue quality can influence healing potential, repair complexity, and long-term strength.



Part of the muscle has been replaced by fatty tissue. This can reduce strength and affect the likelihood of full recovery after repair.
If you have significant fatty atrophy, a reverse shoulder replacement may help you feel and function better.

*Same-week consultations may be available


Even though an MRI provides valuable structural information, it does not establish a complete diagnosis. A rotator cuff tear must be interpreted in the context of strength, movement quality, symptom behavior, and the physical demands placed on your shoulder — both now and over time.

Â
A shoulder specialist integrates these factors through comprehensive evaluation before defining the most appropriate path forward.

Natural healing is unlikely.
Â
Tendons anchor muscles to bone, hence when a rotator cuff tendon tears, the muscle pulls on the tendon causing it to retract—much like a snapped rubber band.
Â
Without proper treatment, this can lead to ongoing pain, weakness, and loss of function.
Â
A comprehensive evaluation by a shoulder specialist can help determine the best path forward.
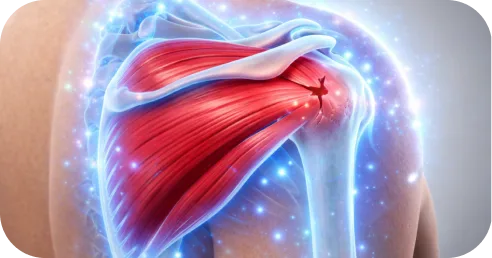
Rotator cuff tears vary in behavior. Some remain stable for years; others enlarge gradually.

Â
Risk of progression increases with greater tear thickness, compromised tissue quality, age, and higher shoulder demands — particularly in tears involving more than 50% of the tendon.
When a tear increases in size, structural changes may develop:
Â
Â
These changes may translate into functional limitations:

Â
In daily life

Â
Â
Sports & performance

Â
Â
As retraction advances or muscle quality declines, restoring durable strength can become more complex and healing potential may decrease.

Appropriate treatment for a rotator cuff tear depends on multiple factors, including tear characteristics, mechanism of injury, shoulder demands, and short- and long-term goals.
For many patients — particularly those with non-traumatic or partial-thickness tears — structured physical therapy can significantly reduce pain and improve shoulder function.
It is important, however, to understand what therapy can and cannot accomplish.
A well-designed rehabilitation program can:
Â
Â
Many patients experience measurable improvement within 6–12 weeks when therapy is structured and progressive.

Physical therapy alone may be less appropriate when:
Â
Â
In these cases, delaying structural repair may increase the risk that the tear becomes more complex over time.
Â
For working adults and athletes, the decision to move beyond therapy is often practical: the shoulder is no longer meeting the demands of work, training, or daily activity. If strength has not returned after a structured rehabilitation program, or relief from injections is becoming shorter, this typically reflects the limits of non-surgical care — and may indicate that structural repair is needed to restore reliable function.

A comprehensive evaluation can determine whether structured rehabilitation is appropriate for your specific tear — and what type of program is most likely to be effective.
Arthroscopic rotator cuff repair reconnects the torn tendon to the bone.
Â
If the tendon is fully detached, it is secured back to its original attachment site.
Â
If the tear is deep but not completely separated, the damaged portion is repaired to restore structural support.

When the tendon heals back to bone:
Â
Â
For many patients, successful repair results in:
Â
Â
Outcomes depend on tear characteristics, tissue quality, timing of repair, structured rehabilitation, and the surgeon’s experience in managing rotator cuff tears.

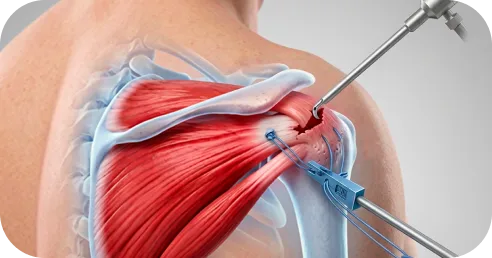
Rotator cuff repair is performed arthroscopically through small incisions using a specialized camera to visualize the shoulder.
Â
The procedure is typically done under regional anesthesia with sedation or general anesthesia.
Â
During surgery, the surgeon:
Â
Small anchors — typically made of biocomposite or titanium — are placed into the prepared bone surface at the tendon’s original attachment site. Strong sutures threaded through these bone anchors secure the tendon back to the footprint under controlled tension.
Â
At The Joint Preservation Center, the fixation configuration is selected based on tear pattern and tissue quality.
Â
For many full-thickness tears, a double-row fixation technique is used. Double-row repair distributes tension across a broader footprint contact area compared to single-row fixation, which can improve initial repair strength and support biological healing. For certain tear patterns, a single-row construct may be more appropriate and equally effective. The choice between single-row and double-row fixation is determined during surgery based on the specific characteristics of your tear.
Â
Incisions are typically only a few millimeters in size. Because the procedure is performed through small incisions using a camera and specialized instruments — sometimes called keyhole surgery — tissue disruption is minimized, which supports faster early recovery compared to traditional open approaches.
The procedure generally takes one to two hours, depending on complexity.
Healing then occurs gradually over several months as the tendon integrates into the bone.
Pain and Early Recovery After Surgery
Â
Most patients experience moderate discomfort in the first several days, which is managed with a combination of regional anesthesia, oral medication, and icing.
Â
A sling is worn to protect the repair, typically for several weeks depending on tear size and tissue quality. The purpose of the sling is to prevent early strain on the healing tendon.
Â
Pain typically improves steadily over the first 1–2 weeks.
Â
Sleeping is often most comfortable in a slightly upright position during the early phase.
Rotator cuff repair heals in phases.
Although the tendon is secured during surgery, biological healing to the bone takes time — and protection during early recovery is essential.
Â
Recovery progresses in structured stages:
Â
Phase 1: Protection and Passive Motion (Weeks 0–4/6)
Gentle, guided movement begins early to prevent stiffness while protecting the repair. The repaired tendon is not yet strong.
Â
Phase 2: Active Motion (Weeks 4/6–8/10)
You begin moving the shoulder under your own power as healing progresses.
Â
Phase 3: Strengthening (After ~10–12 Weeks)
Controlled strengthening begins once the tendon has biologically started to integrate into the bone.
Â
Strength, endurance, and control are rebuilt gradually.

Drive?
Usually when you are out of the sling and off narcotic pain medication.
Â
Return to desk work?
Often within 1–2 weeks, depending on comfort.
Â
Return to manual labor?
Typically several months, depending on demands.
Â
Return to sports?
Non-contact activities may resume gradually around 4–6 months. Overhead or high-demand sports often require 6 months or longer.
Â
Timelines vary based on tear size, tissue quality, and healing response.
Â
Full strength recovery can continue improving for up to a year.
Successful recovery depends on:
Â
Longitudinal studies show that untreated tears can:
These biological changes may reduce healing potential and increase repair complexity later.
Â
This does not mean every tear requires immediate surgery.
Â
It does mean that appropriate timing matters when structural compromise threatens long-term strength.

One of the most common concerns for working adults considering rotator cuff surgery is timing: how to schedule the procedure around professional obligations, minimize income disruption, and plan for the weeks when full function is not yet restored.
Desk work and computer-based roles: Most patients return to desk work within 1–2 weeks, working one-handed or with limited arm use initially. Remote work may allow an even earlier transition. Typing with both hands generally becomes comfortable within 3–4 weeks.
Supervisory, managerial, or client-facing roles: If your work does not require physical lifting, return within 1–2 weeks is typical. Driving is usually possible once the sling is discontinued and you are off narcotic medication, generally within 2–4 weeks.
Manual labor, construction, trades, or physical occupations: Return to light duty may be possible within 2–3 months. Return to full overhead or heavy lifting duties typically requires 4–6 months depending on tear complexity and healing progress. Some employers offer modified duty during this transition.
Work restrictions documentation: We provide work restriction letters and return-to-work clearance documentation as needed for your employer or occupational health department.
Return-to-sport timelines depend on the demands of your activity, the complexity of your repair, and your progress through rehabilitation milestones. Below are approximate ranges for common activities:
These timelines are approximations. Your specific return-to-sport plan is developed collaboratively between your surgeon and your physical therapist based on objective strength milestones.
Preparing your home and support system before surgery helps the early recovery period go more smoothly. Because you will be in a sling and restricted from using your operative arm for several weeks, some advance planning makes a meaningful difference:
Â
Recovery after rotator cuff repair can vary significantly depending on the size and location of your tear, the quality of the tissue, and the specific surgical technique used.
Â
While general timelines can be helpful for orientation, your recovery plan will be personalized. Your surgeon will guide you through a protocol tailored to your shoulder, your goals, and your lifestyle.
Week 1: Sling wear at all times. Pain management with medication, icing, and rest. Begin gentle pendulum exercises as directed. Most discomfort resolves significantly by day 5–7.
Â
Weeks 2–3: First postoperative visit. Passive range-of-motion exercises with a therapist begin. Pain continues to improve. Desk work may resume if comfortable.
Â
Weeks 4–6: Gradual progression of passive and assisted motion. Sling is typically discontinued around week 4–6 depending on tear size and repair security. Driving may resume once the sling is off and narcotic medication is no longer needed.
Â
Weeks 6–10: Transition from passive to active motion. The shoulder begins moving under its own power. Daily activities become noticeably easier.
Â
Weeks 10–16: Strengthening begins. Controlled resistance exercises rebuild rotator cuff and scapular strength. Light recreational activity may resume.
Â
Months 4–6: Progressive strengthening and sport-specific or job-specific rehabilitation. Many patients return to most activities during this window.
Â
Months 6–12: Continued strength gains. Full recovery and confidence with demanding activities. Strength can continue improving for up to a year after surgery.

Not every rotator cuff tear can be addressed with a straightforward arthroscopic repair. Massive tears, irreparable tears, multi-tendon involvement, combined shoulder pathology, and failed prior repairs each present distinct surgical challenges that require advanced techniques and specialized experience.
At The Joint Preservation Center, we evaluate the full spectrum of rotator cuff pathology and offer the appropriate procedure for your specific tear, instead of a one-size-fits-all approach.
When a massive rotator cuff tear cannot be directly repaired because the tendon has retracted too far or the tissue quality is too compromised for reliable healing, superior capsule reconstruction may offer an alternative to replacement.
Â
SCR restores the superior restraint of the shoulder by placing a graft — typically a dermal allograft or fascia lata autograft — between the top of the humeral head and the glenoid. This reconstructed capsule re-centers the humeral head in the socket, reducing superior migration and restoring the mechanical environment needed for the remaining rotator cuff muscles to function effectively.
Â
Who Is a Candidate for SCR?

Â
SCR may be appropriate for patients with massive, irreparable rotator cuff tears who still have intact deltoid function and do not yet have advanced arthritis (cuff tear arthropathy). It is particularly relevant for younger, active patients who want to avoid or delay reverse shoulder arthroplasty and preserve their native joint.
Â
Typical candidates include working-age adults with massive supraspinatus and infraspinatus tears that have retracted beyond direct repair, who still demonstrate functional deltoid and subscapularis activity, and whose imaging does not show significant glenohumeral joint destruction.
Â
SCR Recovery for Active Adults

Â
Recovery after SCR follows a similar phased rehabilitation protocol to standard rotator cuff repair, though the timeline may be somewhat longer given the complexity of the reconstruction. Most patients are in a sling for approximately 6 weeks, with passive motion beginning in the early postoperative period. Active motion typically begins around 6–8 weeks, and strengthening progresses after approximately 12 weeks.
For working adults, return to desk work is generally possible within 2–3 weeks. Return to manual labor or overhead work typically requires 5–7 months depending on demands. Return to sport varies by activity but commonly ranges from 6–9 months.

When a rotator cuff tear is truly irreparable — meaning the tendon cannot be mobilized back to bone even with advanced release techniques — a tendon transfer can restore lost shoulder function by rerouting a nearby muscle-tendon unit to take over the role of the torn rotator cuff.
Types of Tendon Transfers

Â
Latissimus Dorsi Transfer: Used to restore external rotation and overhead function in patients with irreparable posterosuperior cuff tears (supraspinatus and infraspinatus). The latissimus dorsi tendon is detached from the upper arm and transferred to the greater tuberosity to substitute for the torn rotator cuff tendons.
Lower Trapezius Transfer: An alternative for restoring external rotation, particularly when the latissimus dorsi is not suitable or when a more anatomic line of pull is needed. The lower trapezius tendon is transferred with an allograft extension to the rotator cuff footprint.
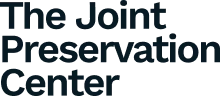
Pectoralis Major Transfer: Used to restore internal rotation and anterior stability in patients with irreparable subscapularis tears. The pectoralis major tendon is transferred to the lesser tuberosity to substitute for the torn subscapularis.
Who Is a Candidate for Tendon Transfer?

Â
Tendon transfers are typically considered for active patients who are not candidates for direct repair or SCR, and who are too young or too active for reverse shoulder arthroplasty to be the preferred option. The decision between tendon transfer types depends on which tendons are irreparable, the patient’s functional demands, and the condition of the remaining rotator cuff.
Recovery and Working-Age Outcomes

Â
Tendon transfers require a structured rehabilitation program that allows the transferred tendon to heal and the patient to retrain the muscle in its new role. Sling immobilization is typically 6 weeks, with progressive motion and strengthening over 4–6 months. Most working-age patients return to daily function within 3–4 months and to sport or heavy labor within 6–9 months, depending on the transfer type and demands.
Many rotator cuff tears do not occur in isolation. Imaging frequently reveals concurrent pathology — a biceps tendon tear alongside a rotator cuff tear, a labral tear accompanying a cuff injury, bone spurs contributing to impingement, or AC joint disease adding to shoulder pain. When multiple structures are compromised, addressing only the rotator cuff may leave residual symptoms.

Rotator Cuff Repair with Biceps Tenodesis

Â
The long head of the biceps tendon runs through the shoulder joint directly adjacent to the rotator cuff. In many rotator cuff tears — particularly those involving the subscapularis or the rotator interval — the biceps tendon is also damaged, inflamed, partially torn, or unstable.
Â
When biceps pathology is present, we may perform a biceps tenodesis at the time of rotator cuff repair. This involves detaching the damaged biceps tendon from its anchor inside the joint and securing it to a new position on the humerus, which eliminates the intra-articular source of pain while preserving biceps strength and cosmesis. Combining these procedures in a single operation avoids the need for a second surgery and addresses all contributing pain generators at once.

Rotator Cuff Repair with SLAP Repair

Â
A SLAP tear involves the superior labrum — the cartilage ring at the top of the shoulder socket where the biceps tendon anchors. In overhead athletes and patients with traumatic shoulder injuries, a SLAP tear may coexist with a rotator cuff tear.
Â
When both structures are compromised, addressing the rotator cuff alone may leave instability or pain from the unrepaired labrum. We evaluate each case to determine whether the SLAP tear requires repair, debridement, or biceps tenodesis, and performs the appropriate combined procedure to restore both cuff integrity and labral stability.
Rotator Cuff Tear with Bone Spurs or AC Joint Pathology

Â
Bone spurs on the undersurface of the acromion can contribute to rotator cuff impingement and may have played a role in the development of the tear itself. Similarly, AC joint arthritis or osteolysis can cause pain that overlaps with and exacerbates rotator cuff symptoms.
Â
When imaging or intraoperative findings confirm concurrent bone spur formation or AC joint pathology, these can be addressed during the same arthroscopic procedure. Subacromial decompression removes impinging bone, and a distal clavicle excision (Mumford procedure) addresses symptomatic AC joint disease — all performed arthroscopically alongside the rotator cuff repair.
Some patients present with rotator cuff tears in both shoulders. Bilateral involvement is particularly common in patients with degenerative tears and can create significant functional limitations when both sides are symptomatic.
Â
Bilateral surgery is typically staged — one shoulder is repaired first, and the second shoulder is addressed after the first has recovered sufficiently for the patient to manage daily activities. We develop a surgical and rehabilitation plan that sequences bilateral repairs to minimize cumulative downtime, which is especially important for working adults managing career obligations and caregiving responsibilities.
A rotator cuff repair that does not heal — whether due to a structural retear, biological failure, or incomplete initial repair — can leave patients with persistent pain, weakness, or declining function. For working adults, a failed primary repair is especially disruptive because the recovery investment (time off work, lost income, months of rehabilitation) has already been made.
Â
When Is Revision Surgery Appropriate?

Â
Revision rotator cuff surgery may be considered when imaging confirms a structural retear or repair failure, symptoms have not resolved after adequate postoperative rehabilitation, and the remaining tissue quality and tear pattern suggest that a second repair has a reasonable chance of healing. At The Joint Preservation Center, we evaluate revision cases with advanced imaging and a thorough assessment of what may have contributed to the initial failure — including tissue quality, fixation adequacy, rehabilitation adherence, and patient biology.
Â
Signs of Repair Failure to Watch For

Â
Patients should be aware of potential signs that a repair may not be healing as expected: a sudden return of weakness after an initial period of improvement, inability to progress through rehabilitation milestones, a specific re-injury event with immediate loss of function, or persistent pain beyond what is expected for the stage of recovery. Any of these warrant reevaluation.
Â
Revision Approaches

Â
Depending on the revision scenario, we may perform a re-repair of the tendon using enhanced fixation techniques, augment the repair with biologic or synthetic scaffolding, convert to a superior capsule reconstruction if direct repair is no longer viable, perform a tendon transfer, or recommend reverse shoulder arthroplasty if cuff tear arthropathy has developed. The revision plan is determined by what the tendon and joint can support at the time of reevaluation.
Cuff tear arthropathy is a distinct condition that develops when a longstanding, massive rotator cuff tear leads to progressive joint destruction. Over time, the loss of the rotator cuff’s centering effect allows the humeral head to migrate superiorly, causing abnormal wear patterns, cartilage loss, and eventually arthritis. This is not simply a “big rotator cuff tear” — it is a structural transformation of the joint itself.
Â
When Reverse Shoulder Arthroplasty Is the Right Option

Â
For patients with established cuff tear arthropathy — where the joint has deteriorated beyond what repair or reconstruction can restore — reverse shoulder arthroplasty (RSA) may be the most appropriate path to pain relief and functional improvement. RSA reverses the normal ball-and-socket relationship of the shoulder, allowing the deltoid muscle to power arm elevation even in the absence of a functional rotator cuff.
Â
At The Joint Preservation Center, our approach is to exhaust all repair and reconstruction options before recommending replacement. Reverse shoulder arthroplasty is reserved for situations where the joint has progressed beyond the point where native tissue restoration is viable.
Â
For working-age patients, this decision carries particular weight. Implant longevity, activity restrictions, and the potential for future revision surgery are all discussed in detail so you can make a fully informed decision about your shoulder’s long-term trajectory.


Modern arthroscopic repair techniques are associated with:
High rates of pain improvement
Significant gains in strength
Improved functional outcome scores
High patient satisfaction
1
We evaluate your symptoms, shoulder strength and movement, review any imaging, and consider your goals and lifestyle. If needed, MRI or ultrasound can be ordered.
2
We explain whether rehabilitation or surgical repair is appropriate based on your tear, shoulder function, and goals.
3
If surgery is recommended, our fellowship-trained shoulder surgeons perform minimally invasive arthroscopic repair to reconnect the tendon to the bone and restore shoulder stability.
4
Our surgeons work closely with physical therapists to guide a structured rehabilitation program that restores motion and strength while protecting the repair.
5
Rehabilitation progresses through milestones so you can confidently return to the activities that matter most — work, exercise, and sport.
This long-term follow-up helps us understand how shoulders recover beyond the early healing period — including strength, function, and return to activity. These insights allow our surgeons to continually refine surgical planning and rehabilitation strategies to support durable shoulder
performance over time.

1
Elite surgeons with decades of experience, incentivized to do the right thing
2
Prevent future surgeries
3
Heal with advanced, minimally invasive techniques
4
Preserve your natural joints, whenever possible
5
Seamless coordination from injury to recovery
6
Premium personalized care, made accessible
7
All patient outcomes tracked for 5 years
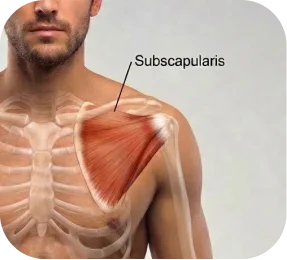
The shoulder rotator cuff is a group of four tendons that connect shoulder muscles to the upper arm bone.
Â
These tendons work together to:
Â
Â
The four rotator cuff tendons are:
Â
Â
When one of these tendons tears, the shoulder can lose strength and stability, which may affect everyday activities and sports performance.
Rotator cuff tears can cause several symptoms depending on the size of the tear and how it affects shoulder function.
Â
Common symptoms include:
Â
Â
Some tears develop gradually, causing progressive pain and weakness over time. Others occur suddenly after an injury and may lead to noticeable loss of strength.
Rotator cuff tears are typically diagnosed by an orthopedic surgeon who specializes in shoulder conditions, often called a shoulder or sports medicine specialist.
Â
During the evaluation, the surgeon reviews your symptoms and performs a physical exam to assess shoulder strength, movement, and pain patterns that may indicate rotator cuff dysfunction.
Â
Imaging studies are then used to confirm the diagnosis and better understand the structure of the tendon:
Â
Â
Because imaging findings do not always perfectly match symptoms, the final diagnosis is based on a combination of physical examination, imaging, and how the shoulder is functioning.
Rotator cuff tears are treated by orthopedic surgeons who specialize in shoulder and sports medicine conditions.
Â
If you are looking for the highest level of specialization, look for a fellowship-trained shoulder surgeon.
Â
Fellowship training is an additional year of advanced surgical training completed after orthopedic residency. During this period, surgeons focus specifically on complex shoulder conditions and procedures such as rotator cuff repair.
Â
This training typically includes:
Â
Â
Because of this focused training and surgical exposure, fellowship-trained shoulder surgeons often have deeper experience in rotator cuff repair and shoulder preservation procedures.
Patients do not feel pain during rotator cuff surgery. The procedure is typically performed under regional anesthesia with sedation or general anesthesia, so the shoulder is completely numb during the operation.
Â
After surgery, some discomfort is expected — particularly during the first 48–72 hours, when the initial inflammatory response is strongest. Pain is usually managed effectively with a combination of medication, ice, sling support, and activity modification.
Â
Many patients also receive a regional nerve block, which can keep the shoulder numb for several hours after surgery and help make the first day significantly more comfortable.
Â
Sleeping can feel awkward at first because the shoulder must be protected in a sling. Many patients find it more comfortable to sleep slightly upright or supported with pillows during the first couple of weeks.
Â
As healing progresses, pain typically improves steadily over the following weeks. Structured rehabilitation then helps restore motion and strength while protecting the repair.
Â
For many patients, the short-term recovery period is worthwhile because successful repair can restore strength, reduce pain, and allow a return to activities that were previously limited by the tear.
Arthroscopic rotator cuff repair is a reliable procedure for appropriately selected patients, especially when the tear is repairable, tissue quality is adequate, and rehabilitation is followed closely. The strongest predictor of success is healing of the repair: the AAOS 2025 Clinical Practice Guideline states that healed rotator cuff repairs show better patient-reported and functional outcomes than physical therapy alone or repairs that do not heal.
Â
Outcomes vary with:
Â
Â
In general, smaller and medium-sized tears heal more reliably, while large or massive tears carry higher re-tear risk. Recent literature cited in 2025–2026 publications reports re-tear rates of roughly 5% to 10.3% for small/medium tears and substantially higher rates for large/massive tears, commonly around 37% and, in some series, near 50%.
Â
From the patient’s perspective, success is usually measured by more than tendon healing alone. Most patients want to know whether pain improves, strength returns, and the shoulder becomes reliable again. Long-term studies show that arthroscopic repair is associated with favorable functional outcomes, high satisfaction, and low revision rates at 10 years or more, although structural re-tears can still occur, especially in larger tears.
Â
For active patients, return to sport or higher-demand activity is also an important marker of success. A 2024 review reported that about 75% of patients returned to sport after arthroscopic rotator cuff repair, at an average of 6.4 months, although return rates vary by sport, tear pattern, and level of competition.
Â
At The Joint Preservation Center, our surgeons track outcomes for 5 years because the true success of rotator cuff repair is not just early pain relief — it is whether the shoulder remains strong, functional, and durable over time.
Â
Evidence & References
Â
AAOS Clinical Practice Guideline – Management of Rotator Cuff Injuries (2025); Moosmayer et al., JBJS; Contemporary JBJS/AJSM Long-Term Studies on Functional Outcomes and Healing; Recent Meta-analyses on Retear Risk by Tear Size (2024–2025).
Recovery after rotator cuff repair occurs in phases because the tendon must heal back to the bone.
Â
Most patients wear a sling for several weeks to protect the repair while early healing takes place. During this time, gentle guided motion is introduced to keep the shoulder mobile without stressing the repair.
Â
Over the following weeks, rehabilitation gradually progresses to strengthening exercises as the tendon continues to heal.
Â
Many patients regain meaningful day-to-day function within 3–4 months. However, full recovery of shoulder strength, endurance, and confidence with higher-demand activities can continue improving for 6 months or longer, depending on the size of the tear, tissue quality, and the demands placed on the shoulder.
Â
A structured rehabilitation program and adherence to recovery guidelines play an important role in achieving the best possible outcome.
Unlike rotator cuff repair (which preserves native tissue), shoulder replacement involves implanting metal and polyethylene components.
Shoulder replacement can be effective for advanced arthritis or irreparable rotator cuff tears. However, it is a major reconstructive procedure and carries different risks than rotator cuff repair.
Potential risks include:
Younger and more active patients place greater stress on implants, which may affect long-term durability.
Yes, many people can still move their shoulder even when a rotator cuff tear is present.
Â
Other muscles around the shoulder can temporarily compensate for the torn tendon, allowing the arm to move. However, this compensation often comes with reduced strength, fatigue, or pain during certain movements.
Â
Over time, continued strain on the remaining tendon fibers may lead to worsening weakness or progression of the tear in some cases.
Rotator cuff tears can occur either suddenly from an injury or gradually over time.
Â
Traumatic tears often happen after a fall, lifting injury, or shoulder dislocation. Patients typically notice immediate pain and weakness.
Â
Degenerative tears develop gradually as the tendon weakens with age, repetitive use, or reduced blood supply to the tissue. These tears may cause slowly increasing pain and weakness over months or years.
Â
Both types can affect shoulder strength and stability.
Pseudoparalysis refers to the inability to actively lift your arm despite having intact nerve function. It occurs when a massive rotator cuff tear is so extensive that the remaining muscles cannot generate enough force to elevate the arm against gravity. Patients often describe their arm as “completely weak” or say they “can’t raise” their arm at all.
Â
Pseudoparalysis is an important clinical finding because it typically indicates a massive or multi-tendon tear that may require advanced surgical intervention such as superior capsule reconstruction, tendon transfer, or in some cases, reverse shoulder arthroplasty. If you are experiencing this level of weakness, evaluation by a shoulder specialist experienced in complex tear management is recommended.
Yes. It is common for MRI to reveal concurrent pathology alongside a rotator cuff tear, including bone spurs (subacromial impingement), biceps tendon tears or instability, SLAP tears (superior labral tears), and AC joint arthritis or osteolysis.
Â
We routinely address combined shoulder pathology during a single arthroscopic procedure. For example, rotator cuff repair can be combined with biceps tenodesis, SLAP repair, subacromial decompression, or distal clavicle excision depending on what your imaging and intraoperative findings indicate. Addressing all contributing structures in one operation avoids the need for a second surgery and typically produces better overall outcomes.
Bilateral rotator cuff tears are managed with a staged approach — one shoulder is repaired first, and the second is addressed after the first has recovered sufficiently for you to manage daily activities comfortably. We develop a sequencing plan that minimizes total downtime, which is especially important for patients managing work obligations and family responsibilities.
The Joint Preservation Center accepts most PPO insurance plans that have out-of-network benefits:
Â
If you have a PPO insurance plan with out-of-network benefits:
Â
Â
Note: If you have Medicare, Medicaid, TRICARE, or VA programs, or if your PPO does not have out-of-network benefits, you can still see our specialists and the surgery center will still be in-network. In this case, our specialists charge $250 for the initial office visit (all follow ups are included). Surgery is typically in the range of $6K – $8K depending on what you need done.
Â
If you are unsure whether your plan is accepted, our team can verify your coverage before your appointment.
*Same-week consultations may be available